
Introduction: The Foot & Ankle
The foot and ankle are specially designed to transmit the body’s weight. The foot is capable of adjusting to cope with various terrains. The arrangement of the bones, ligaments and fascia give a spring-like arch structure and there are thick pads under the heels and toes – together they act as shock absorbers.
The foot and ankle are targets for various arthropathies and also, because of the concentrated stresses on the joints, there can be other problems.
Anatomy of the foot and ankle
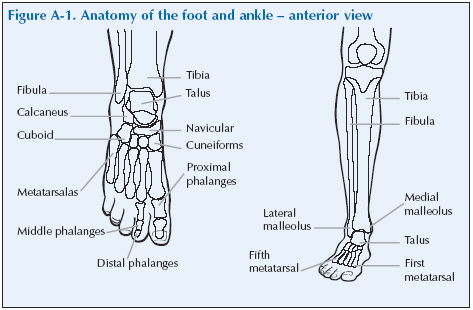
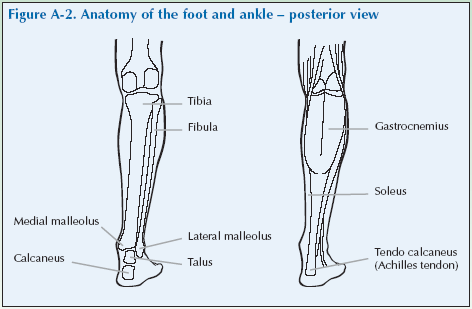
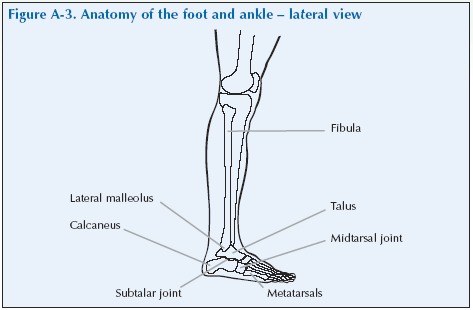
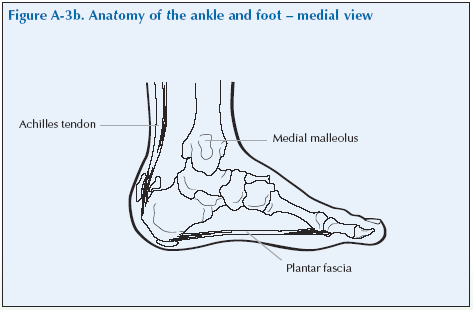
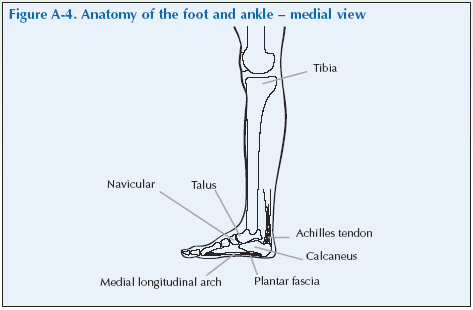
The ankle joint is found where the tibia and fibula meet the talus bone of the foot. The talus bone articulates with the calcaneus (heel bone) at the subtalar joint. The Achilles tendon is attached to the calcaneus. The lateral and medial malleoli are the widest projections at either side of the ankle.
The foot contains seven bones called the tarsals (together called the tarsus), five metatarsals (the long bones of foot), as well as five phalanges (toes). The joints between the tarsals and metatarsals are the tarsometatarsal joints. Taken together, the articulation between the tarsus and metatarsals is called the midtarsal joint. The articulation between the metatarsals and the phalanges are the metatarsophalangeal (MTP) joints.
Each toe has three phalanges except the big toe which has two. The medical term for the big toe is the hallux. The joints in the toes are the proximal interphalangeal and distal interphalangeal joints. The big toe has one interphalangeal joint.
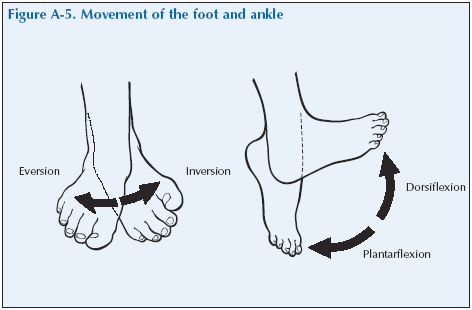
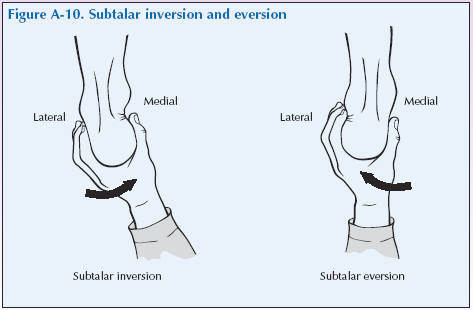
There are some special terms that relate to movement of the foot. These are inversion which means lifting the medial border of the foot and eversion, which is lifting the lateral border. (Inversion is holding your foot out in front and making your big toe point up while your little toe points down; eversion is the opposite).
Dorsiflexion or just flexion involves moving the top of the foot towards the shin and plantar flexion or extension, is the opposite movement otherwise known as pointing your toes down.
Movement of the midtarsal joint is rotation.
The toes can be flexed, extended, abducted and adducted
Problems of the foot and ankle
Articular causes
[su_table]
| Osteoarthritis | Commonly affects the first MTP joint |
| Inflammatory arthritides | Rheumatoid arthritis |
| Gout – typically affects the first MTP joint
Psoriatic arthritis – typically affects the toes as a whole to cause sausage-like swelling |
[/su_table]
Periarticular causes
[su_table]
| Plantar fasciitis | |
| Achilles tendonitis
Achilles tendon rupture |
|
| Bursitis | Retrocalcaneal and retroachilleal bursitis |
| Enthesopathy | Ankylosing spondylitis
Reactive arthritis (Reiter’s Syndrome) Psoriatic arthritis |
[/su_table]
Trauma
[su_table]
| Sprain | |
| Fracture |
[/su_table]
Biomechanical defects
[su_table]
| Flat feet |
[/su_table]
Biomechanical problems of the foot are common as it is a complex mechanical structure that is under a lot of physical stress, carrying the body’s weight and adjusting to all terrains. They sometimes cause pain. Flat feet, or loss of the medial longitudinal arch with pronation of the foot on weight-bearing is the commonest.
Injuries of the ankle are extremely common. These are usually of the periarticular structures, often called soft tissue injuries. In severe cases they can be difficult to distinguish from fractures.
Achilles tendon problems are sometimes seen, particularly in athletes such as runners and jumpers, but also in people who play football or tennis and ballet dancers. There may be inflammation of the tendon insertion or of the tendon. The tendon can rupture, either partially or fully. These problems give rise to localised pain at the back of the heel, often going into the calf related to lower limb activity. There may be weakness of plantarflexion.
Plantar fasciitis is inflammation of the tissues of the plantar fascia where it joins the heel or calcaneus.
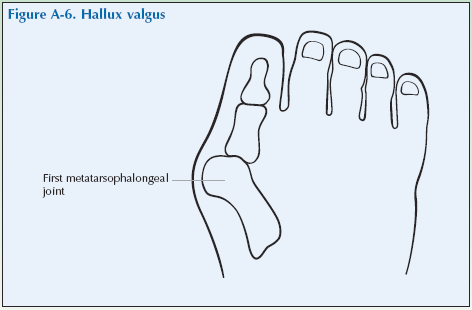
Osteoarthritis of the first MTP joint is common. The joint becomes prominent (a bunion) due to bony swelling and also because of valgus deformity of the hallux. Osteoarthritis of the ankle is rare, but may sometimes be seen after ankle fractures.
Rheumatoid arthritis commonly affects the MTP joints from an early stage. Swelling of the MTP joints results in spreading of the toes so that daylight can be seen between them. The spread of the front of the foot is also accompanied by loss of the medial longitudinal arch. This can put stress on the ankle which can be painful and an eversion deformity may develop. Involvement of the ankle joint itself is not uncommon but is seldom seen as the first sign of the disease.
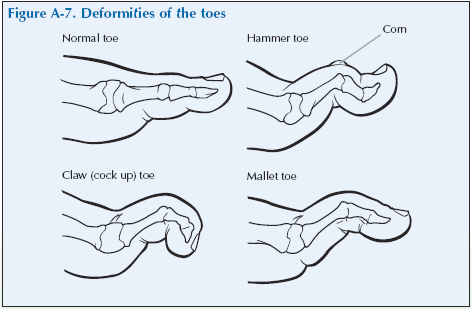
Common deformities of the toes are:
Claw toe: The MTP joint is hyperextended and both the proximal and distal interphalangeal joints have flexion contractures.
Hammer toe: The MTP and the distal interphalangeal joints are hyperextended and the proximal interphalangeal joint has a flexion contracture.
Hallux valgus: Commonly known as a bunion, it is characterised by a medial displacement of the first metatarsal and a lateral deviation of the first phalanx or big toe.
Giving a history of foot and ankle problems
Invite the docor to carry out a consultation by first asking you about your history related to the experience you have of your condition. This will then be followed by the physical examination.
The doctor should first ask you ‘What is the problem?’ and you should give a short response describing your symptoms and their effect on your quality of life.
Develop a script based on your own experience. You may still have the symptoms or you may be describing an episode you have had as if it were still present.
Describe as fully as you can your own symptoms, including where in and around the ankle and foot you feel/felt pain or discomfort. Say if you have any stiffness, swelling or other symptoms. Mention how the problem is having/had an impact on your daily life, your work or your sleep.
Remember to describe how your condition affects/affected your quality of life. Consider self care (e.g. ability to wash, dress, toilet and feed), domestic care (e.g. ability to cook, clean, launder, shop), work (e.g. ability to stand, sit, type), leisure (e.g. ability to play sports, walk, go out for meals). Explain about the way it limits/limited your activities and restricts/restricted your participation in normal life.
Do not tell him everything spontaneously – just the important part. He will then need to ask further questions to fully characterise your problem. Develop a set of answers with your trainer to the following points. Prompt them if they omit important questions.
Pain is usually present and questions should establish:
- How the pain started and developed.
- The nature of the pain.
- The exact distribution of the pain.
- Whether the pain has increased or decreased over time.
- Whether it affects sleep.
- Whether anything exacerbates or relieves the pain. Stiffness may be a symptom and questions should establish:
- If you are stiff at all?
- When it is worse?
- What improves it?
Swelling may be a symptom and questions should establish:
- If you have noticed any swelling and where.
- If it is always present.
- If it is painful or tender.
- If it is increasing.
They need to ask about the pattern of all the symptoms – where they started and if they have spread anywhere.
You may prompt the doctor (if you have not already told them) to make sure that they include the following information:
- Your age, occupation and hobbies.
- Your general health.
- Your past medical history.
- Whether you have injured or strained your ankle or foot.
- Whether there is any impairment of function and how this impacts on your daily activities and quality of life.
- Ankle and foot problems typically cause difficulty in walking, especially on uneven surfaces, driving and balancing.
- Whether you have had previous treatment and if so whether it was successful.
The effect of any problem depends on your personal circumstances. The doctor needs to know about what you need to do in the home, at work, your leisure interests and your expectations.
You may have symptoms affecting other parts of your musculoskeletal system. You may prompt the doctor to ensure he has asked whether you have any other problems affecting your muscles, joints, neck or back.
You may go into further details about how your problem affects your life and the treatment you have received at the end of the session when discussing the findings.
Example of a Script
You should develop something like this, based on your own story. First you need to ask me: “What is your problem?”
“I am getting pain in my ankles and feet when walking, I feel like I have pebbles in my shoes.”
You should then respond to questions, guiding and prompting the doctor through the information as listed above.
Foot and Ankle Examination Script
Describe the examination to the doctor using the anatomical and directional terms you have learnt. You can use your knowledge of anatomy best when the doctor is feeling the joint and periarticular structures.
“I would now like to invite you to find out a little bit more about my problems, by role play, using me as your patient and examining me.”
Look
Observe the patient standing and walking to look for signs of limitation of movement and misalignment. Note whether walking induces pain. Look to see if they maintain their medial longitudinal arch. Note if there is spreading of the front of the foot.
Inspect the ankle, foot and toes for redness, swelling, soft tissue changes, rheumatoid nodules and alignment changes. Look for changes such as hallux valgus (bunion), claw toe and hammer toe.
Inspect the soles of the feet for any callosites.
What do you see?
Feel
Palpate the area generally for heat.
Palpate the medial and lateral malleoli and along the joint line across the front of the ankle feeling for tenderness and swelling. Palpate the Achilles tendon, feeling for tenderness and soft tissue changes such as rheumatoid nodules, which are quite common in this area.
Palpate the base of the calcaneus feeling for tenderness caused by plantar fasciitis.
Palpate the dorsum of the midfoot for tenderness or swelling.
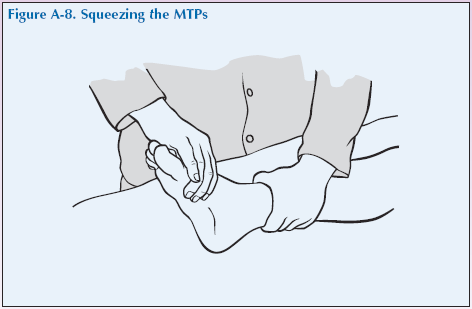
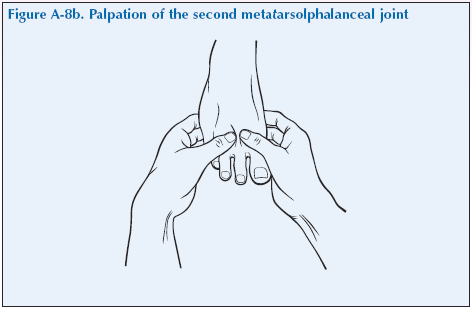
Gently squeeze the metatarsals together (take care as this could be painful for the patient). If this manoeuvre causes pain, there is likely to be inflammation of one or more MTP joint. Each MTP joint should then be palpated individually by pressing with your thumb and finger, feeling for tenderness.
Palpate the proximal and distal interphalangeal joints of the toes, feeling for tenderness. Rheumatoid nodules may also be found on the toes.
What do you feel?
Move
It is best to test movements of the ankle and foot with the knees flexed and legs dangling to relax the muscles of the calf – such as sitting on the edge of the examination couch.
Initially assess the active range of motion by asking them to move their foot and ankle as directed.
Flexion and extension
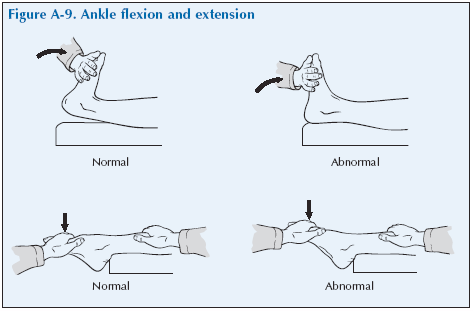
Ask them to dorsiflex their ankle as far as they can without pain. Then ask them to extend (or plantarflex) their ankle as far as they can without pain. This movement is at the ankle joint.
Inversion and supination
Ask them to turn the soles of their feet inwards as far as they can without pain to try and face each other.
Eversion and pronation
Ask them to turn the soles of their feet outwards as far as they can without pain.
Flexion and extension of the toes
Ask them to flex (curl) their toes. Then ask them to extend their toes towards the upper part of the foot.
If these are at all restricted or painful, then test the passive range of motion, still with the leg dangling.
Flexion and extension
To test these movements of the ankle joint, grasp the calcaneum (heel) and with the other hand push the foot into maximum dorsiflexion and then plantar flexion without causing pain.
Inversion and eversion
To test these movements of the subtalar joint, hold the distal leg with one hand to stabilise it and grasp the calcaneum (heel) with the other hand and use it to move the foot into inversion and eversion.
Midtarsal rotation
To test these movements of the midtarsal joint, hold the calcaneum (heel) in one hand and the distal foot with the other and use it to rotate the foot into supination and pronation.
First MTP joint
Hold the first MTP joint between finger and thumb of one hand and the big toe with finger and thumb of the other hand, flex and extend it to assess range, if painful and if crepitus.
Note: range of motion and if any tenderness or pain for all these movements.

What have you found?
Stress
Standing on the toes stresses the Achilles tendon and is a way of testing its status.
Listen
Crepitus may be heard on movement.
Special tests
Foot pain may be neuralgic. A neurological examination should also be done, especially if there are any symptoms of tingling, numbness or weakness in the feet.
Lightly touch the palmar and dorsal surfaces of the feet and toes and ask if sensation is normal. Test strength by asking them to dorsiflex the foot and the hallux against resistance and then plantar flex the foot against resistance. The reflexes in the legs should now be tested (knee and ankle jerks and plantar response).
“We have now come to the end of this mock consultation. You should have learned quite a bit about my condition from taking my history and examining my joints, however, I would be happy to provide you with a bit more detail about the progress of my condition and how it affects my life, if you would find this useful.”
[Please give a brief description of your condition:
- When and how it started.
- Physical and psychological affects on you.
- Treatments offered.
- How your condition progressed.
- How this affected your life: Home, education, work, leisure, ability to travel, relationships etc.]
“Does anyone have any further questions?”
“Thank you again for attending this session. I hope you have found it useful.”