
Introduction: The Shoulder
The shoulder is a complex joint that has remarkable mobility in a number of directions. The glenohumeral joint is extremely mobile and there is a special arrangement of the tendons and ligaments around this joint called the rotator cuff that keeps the joint stable while allowing a large range of movement.
Shoulder problems usually present with pain and it important to distinguish between pain in the joint itself (articular pain), pain in the surrounding soft tissues (periarticular or extra-articular pain) and referred pain.
Anatomy of the shoulder
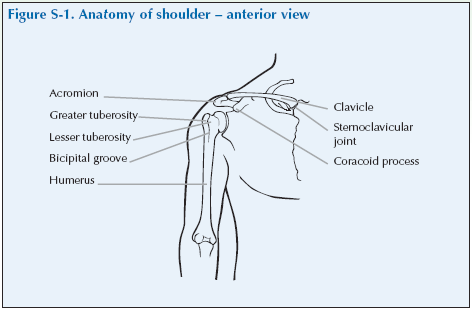
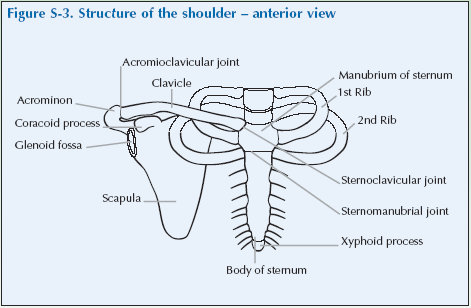
The bones that form the complex shoulder joint are the scapula, clavicle and humerus. The joint itself is a ball and socket joint formed by the head of the humerus and the shallow glenoid fossa of the scapula, whilst the clavicle and the scapula form the shoulder girdle.
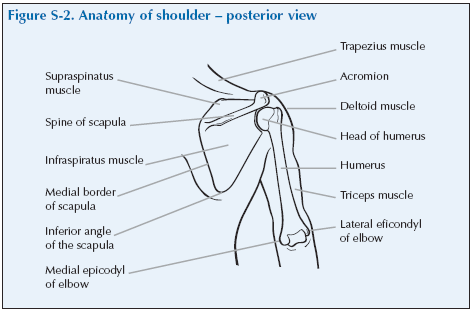
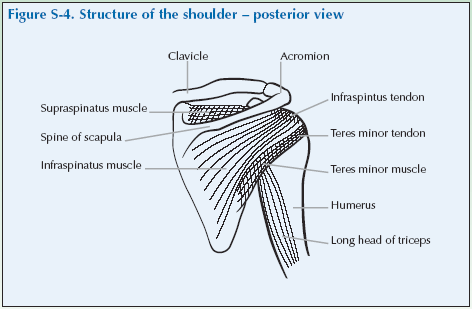
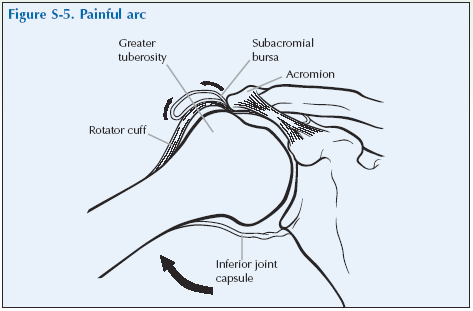
Stability and function of the shoulder are provided by the surrounding soft tissues, including the supraspinatus, the subscapularis, the infraspinatus and the teres minor muscles. The muscles originate from various parts of the scapula and attach to the upper end of the humerus. The tendons of these muscles give added stability to form the rotator cuff as it passes under the acromion process. The rotator cuff is the name given to the four muscles and tendons that encircle the neck of the humerus. The rotator cuff keeps the shoulder joint stable and enables movement of the shoulder.
The acromioclavicular joint, the acromion process and the coracoid process are also important components of the shoulder. The scapula is a triangular shaped bone at the posterior of the shoulder. The spine of the scapular forms a continuous arch ending at the acromion process, which then articulates with the clavicle to form the acromioclavicular joint.
Two other areas that deserve attention are the bicipital tendon located just below the humeral head, in the bicipital groove, and the subdeltoid bursa, which is a closed sac found under the deltoid muscle on the lateral portion of the shoulder.
Problems and causes
Most shoulder problems are due to soft tissue disorders, with rotator cuff lesions (tendinosis and tears) being the most common complaint. Shoulder pain may originate from many different sources, such as the acromioclavicular joint, the subdeltoid bursa and the bicipital tendon.
The common causes of shoulder pain are:
| Perirticular causes | |
| Rotator cuff lesions | There may be inflammation of the tendons (tendinitis), degeneration of the tendon (tendinosis) or actual tears of the cuff, usually of the supraspinatus tendon (tendon rupture, rotator cuff rupture). |
| Impingement | Impingement is squeezing of the supraspinatus tendon between the head of the humerus and the acromion process as the arm is raised. |
| Frozen shoulder or
adhesive capsulitis |
Frozen shoulder is when there is adhesion and shrinkage of the glenohumeral joint capsule. There is shoulder pain, which may be worse at night and limitation of both passive and active movement in all directions (especially external rotation), which can be quite severe and restricting. |
| Articular causes | |
| Osteoarthritis | OA can occur in the glenohumeral joint or is quite common in the acromioclavicular joint |
| Rheumatoid arthritis | RA often affects the shoulders, usually the glenohumeral joint |
| Infection | Infection is an uncommon but important cause.This should always be thought of by the doctor as early diagnosis and treatment is necessary. |
| Referred pain | Pain can be referred to the shoulders from the cervical spine and from the lining of the lung (pleura), diaphragm, gall bladder and heart. |
Giving a history of shoulder problems
Invite the doctor to carry out a consultation by first asking you about your history related to the experience you have of your condition. This will then be followed by the physical examination.
The doctor should first ask you ‘What is the problem?’ and you should give a short response describing your symptoms and their effect on your quality of life.
Develop a script based on your own experience. You may still have the symptoms or you may be describing an episode you have had as if it were still present.
Describe as fully as you can your own symptoms, including where in the shoulder you feel/felt pain or discomfort and whether you have had any tingling in your arms and/or hands. Say if you have any stiffness, swelling or other symptoms. Mention how the problem had/is having an impact on your daily life, your work or your sleep.
Remember to describe how your condition affects/affected your quality of life using the framework covered in the earlier section of this manual. Consider self care (e.g. ability to wash, dress, toilet and feed), domestic care (e.g. ability to cook, clean, launder, shop), work (e.g. ability to stand, sit, type), leisure (e.g. ability to play sports, walk, go out for meals). Explain about the way it limits/limited your activities and restricts/ restricted your participation in normal life.
Do not tell him everything spontaneously – just the important part. He will then need to ask further questions to fully characterise your problem. Develop a set of answers with your trainer to the following points. Prompt them if they omit important questions.
Pain is usually present and questions should establish:
- How the pain started and developed.
- The nature of the pain.
- The exact distribution of the pain.
- Whether the pain has increased or decreased over time.
- Whether it affects sleep.
- Whether anything exacerbates or relieves the pain. Stiffness may be a symptom and questions should establish:
- If you are stiff at all?
- When it is worse?
- What improves it?
Swelling may be a symptom and questions should establish:
- If you have noticed any swelling and where.
- If it is always present.
- If it is painful or tender.
- If it is increasing.
They need to ask about the pattern of all the symptoms – where they started and if they have spread anywhere.
You may prompt the doctor (if you have not already told them) to make sure that they include the following information:
- Your hand dominance.
- Your age, occupation and hobbies.
- Whether you have injured or strained your shoulder or neck.
- Your general health.
- Your past medical history.
- Whether you have any symptoms such as tingling, numbness or weakness in your arms/hands/fingers.
- Whether there is any impairment of function and how this impacts on your daily activities and quality of life.
– Shoulder problems typically produce difficulties in brushing or combing hair, dressing, driving a car, reaching for items from a shelf, playing sports.
- Whether you have had previous treatment and if so whether it was successful.
The effect of any problem depends on your personal circumstances. The doctor needs to know about what you need to do in the home, at work, your leisure interests and your expectations.
You may have symptoms affecting other parts of your musculoskeletal system. You may prompt the doctor to ensure he has asked whether you have any other problems affecting your muscles, joints, neck or back.
You may go into further details about how your problem affects your life and the treatment you have received at the end of the session when discussing the findings.
Example of a Script
You should develop something like this, based on your own story. First you need to ask me: “What is your problem?”
“I have had shoulder pain for several months and it is worse if I try and lift my arm such as when dressing and brushing my hair. It wakes me if I lie on it.”
You should then respond to questions, guiding and prompting the doctor through the information as listed above.
Shoulder Examination Script
Describe the examination to the doctor using the anatomical and directional terms you have learnt. You can use your knowledge of anatomy best when the doctor is feeling the joint and periarticular structures.
“I would now like to invite you to find out a little bit more about my problems, by role play, using me as your patient and examining me.”
Look
Inspect the shoulders and shoulder girdles anteriorly and each scapula and related muscles posteriorly for redness (not often seen), swelling, skin changes, changes in alignment, and muscle wasting.
Changes in alignment can include the appearance of uneven shoulders and/or scapulae. Look at the tips of the shoulders and the tips of the the scapulae.
Look for any prominence of the sternoclavicular joints, clavicles or of the acromioclavicular joints.
Swelling is uncommon. When present, it usually occurs in the glenohumeral joint appearing at the anterior concavity causing the natural gully of the shoulder to disappear or even bulge. It might be easier to see from the side.
Wasting of the deltoid muscles can result in the lateral edge of the proximal end of the humerus becoming prominent and the shoulders having a squared appearance. There may be a flattened or hollow appearance above and/or below the scapula spine.
What do you see?
Feel
Feel the shoulder with the back of your hand for heat laterally, anteriorly, superiorly and posteriorly, but is not often detectable.
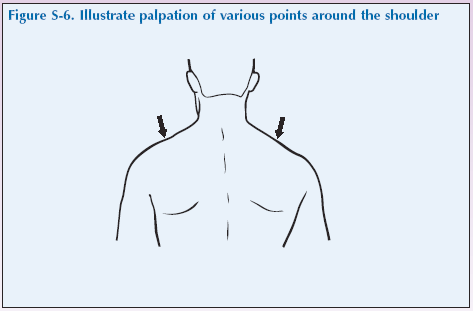
Palpate over the midpoint of each trapezius and the supraspinatus to identify if the muscle is in spasm and for tender spots.
From the front, use your thumbs to feel the sternoclavicular joint and then run your thumb along the clavicle following it out towards the acromion process and feel for the dip, which is the acromioclavicular (AC) joint. Press on the AC joint for tenderness. Ask the patient to roll the shoulder while palpating for pain and crepitation.
Then move your thumb and fingers laterally and feel the tip of the acromium and then the head of the humerus. In the hollow between, deep to the overlying deltoid muscle, is the supraspinatus tendon.
The subdeltoid bursa, if swollen, can be palpated in this gap between the tip of the acromium (acromium process) and the head of the humerus.
Then feel the muscles of the rotator cuff behind the humerus.
Next feel the bicipital tendon which can be found anteriorly just below the acromion overlying the humeral head, in the bicipital groove. It may be difficult to locate the tendon and having the patient rotate the arm externally may make it easier to palpate.
Finally you can feel for the coracoid process which is medial to the biceps tendon.
What do you feel?
Move
The motions of the shoulder girdle are flexion, extension, abduction, adduction, and internal and external rotation.
In the shoulder joint especially, pain on active and passive motion can give crucial information as to the location of the problem – that is whether it is articular or periarticular. Generally, pain that is worse during active movement compared to passive movement suggests periarticular problems such as rotator cuff lesions.
It is easiest if the patient is standing. Stand in front of them to instruct and show if necessary what they should do.
Firstly assess the patient’s range of active movement and identify if any movements are painful and at what points of the range of movement.
There is only a need to perform passive range of motion if a problem was detected with active movements. Assess both shoulders, either separately or both at the same time.
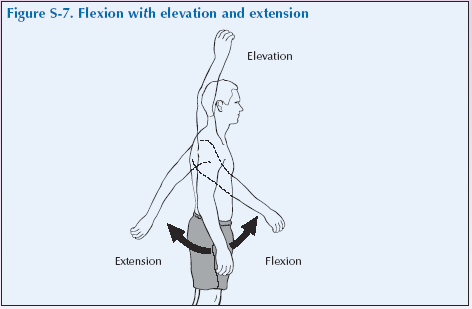
Flexion of the shoulder to elevate the arm – with keeping the arm straight, ask them to lift it forward and up, above the head as far as is comfortable.
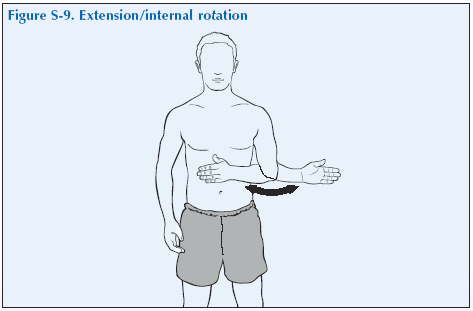
Extension – now ask them to drop their arm down and swing it backwards as far as is comfortable.
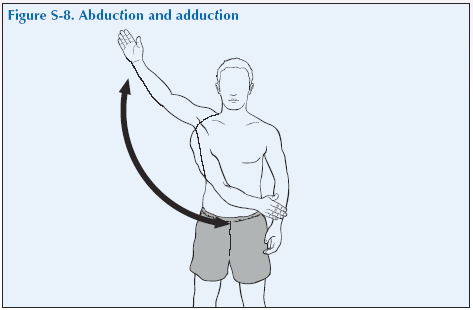
Abduction – ask them to raise their straightened arm out sideways and up above the head as far as is comfortable. Pain between 30 and 120° is called a painful arc.
Adduction – now ask them to lower their arm and swing it across their front, or put their hand behind their back as far as is comfortable which is a fuller test of the range of abduction.
External rotation – with the arm hanging by their side, ask them to flex the elbow to 90° with the hand in a neutral position (palm perpendicular) and to then rotate out their forearm as far as is comfortable.
Internal rotation – now ask them to rotate their arm inwards, still with the elbow at 90° flexion so that the flat of the hand touches the stomach if there is a full range of movement.
Then test some mixed functional movements by asking them to:
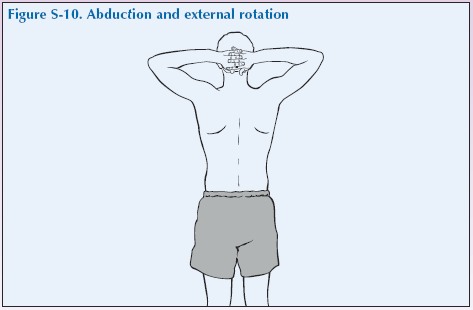
- Abduction and External Rotation – raise up the straightened arm sideways (abduction), and then flex the elbow and place the hand behind neck keeping the neck straight. The patient should then push the elbows back as far as possible without causing too much pain. Doing this with both arms together is part of the Screening Assessment.
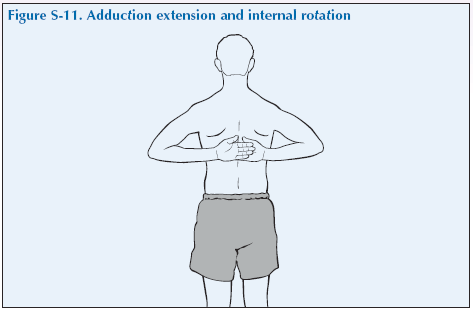
- Adduction, Extension and Internal Rotation – place hands behind the small of the back; and try to touch opposite scapula.
If any of these movements are restricted, then you may repeat them passively, with you guiding the patients arm to establish the maximum range without causing too much pain.
When doing these always watch the patient for non-verbal signs of pain. Support the arm between the joints, holding at the middle of the upper arm and middle of the forearm.
Abduction is at the glenohumeral joint and also by rotation of the scapula. If it is limited you can judge how much movement is occurring at each by holding the scapula to fix it and then asking them to abduct the arm and seeing how much glenohumeral movement there is.
What have you found?
Stress
If there is shoulder pain on abduction, then ask the patient to abduct the shoulder with you resisting it. Pain with movement against resistance at initiation of abduction suggests supraspinatus tendonitis.
Listen
Crepitus may be heard with movement of the shoulder although it is more commonly felt. It may be articular or periarticular, but this is not often of clinical significance.
Special tests
Neurological function should be examined – sensation to light touch over the arms and hands, grip strength and reflexes.
Making a firm grip can cause shoulder pain.
“We have now come to the end of this mock consultation. You should have learned quite a bit about my condition from taking my history and examining my joints, however, I would be happy to provide you with a bit more detail about the progress of my condition and how it affects my life, if you would find this useful.”
[Please give a brief description of your condition:
- When and how it started.
- Physical and psychological affects on you.
- Treatments offered.
- How your condition progressed.
- How this affected your life: Home, education, work, leisure, ability to travel, relationships etc.]
“Does anyone have any further questions?”
“Thank you again for attending this session. I hope you have found it useful.”